Following an operation for an ischaemic leg and femoral posterior in 1980, the patient was asked if she could raise £3,000 to replace a piece of equipment which was held together by sticky tape, but very necessary for Vascular Surgery etc.
This was to be the beginning. The first donation of £100 was given by the husband of the patient and the surgeon gave £175 which had been given to him by previous patients.
Where do we go from here?
A meeting was arranged with members of the Cardiac department, who already had experience with fund-raising. Following this, a Committee of three surgeons, a radiologist and a neurologist was formed with the ex-patient as secretary/fund raiser. Her problems had just begun!
For a short time, the fund was called “The Vascular Fund” but soon realised that this did not have an impact on the general public. Stroke & Circulation had a greater meaning, most people know someone who has had s stroke and could relate to the fund much better.
How to get people interested was a problem. There was lots of publicity and descriptive leaflets of the aims of the Fund printed, but these were not allowed to be placed within the hospital at that time. To get people involved, it was decided to offer a membership of £5 yearly, this being to cover the cost of advertising, postage and information relating to fund raising events. It worked and many people were interested.
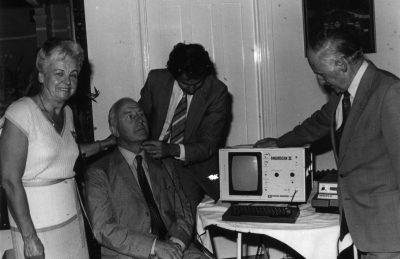
One of the first machines purchased by the Fund being demonstrated by Philip Somerville, Vascular Surgeon.The first fund raising event was held in September 1980 – A cheese and wine party at £2.50 per head and this raised £792! This gave the Committee great encouragement and further small events were held. A small party in the boardroom of the hospital was held together with a Xmas Draw, principally to thank all those who had helped get the fund off the ground. The Xmas Draw and donations raised £501. This enabled the Fund to purchase the first items for the Vascular Unit – arterial cuffs and Doppler flow meters.
There followed a very successful “Open Evening” in co-operation with the Cardiac Department, showing the equipment which the Vascular Department (although there wasn’t one yet) would like the Fund to purchase.
Presentation of scanner to the X-Ray Department in the 1980s. The SSCF raised £12,000 of the £17,000 total cost.The next purchase was a Flowmeter costing £5,000 and this was soon followed by a scanner which had to be located in the X-Ray Department. The Fund paid £12,000 towards the total cost of £17,000, the health authority meeting the balance.
Due to the family of the late Norman Peroni kindly donating £6,000, the Fund was then able to purchase an Angioscan 11 costing £10,000. By now, the Vascular Technician had an office and the Angioscan was housed there. Medical books costing £500 were also purchased and kept in the office for use by the trainee doctors.
Much fund raising took place during this period and the membership part of the Fund was discontinued.
Various pieces of equipment were then purchased for use by the Vascular Surgeons at the Princess Royal Hospital, including a Photoplethysmograph, many hand held Doppler machines for G.P. surgeries, the wards in the Royal Sussex County Hospital and Cuckfield Hospital and a DATEX Cardiocap for the X-Ray Department.
In 1987, the Fund became a Registered Charity – previously it had been part of the endowment fund within the Royal Sussex County Hospital.
The Fund refurbishes the Interventional Radiology SuiteFinally a room was made available for the first Vascular Laboratory – the Fund paid for lots of the smaller pieces of equipment, a Diasonic Ultrasound System and towards some of the work to make the room suitable for purpose.
A large bequest from the estate of Esme Anderson enabled the Fund to pay £150,000 of the £500,000 towards a new Interventional Vascular Suite. Brighton & Hove Lions also contributed £25,000 to this project.
My leg muscles hurt when I walk….
I can’t manage hills without a short stop….
I often need to stop and hang on to a lamp post or pretend to be interested in shop windows….
One in five men over 50 are thought to have some degree of intermittent claudication. Women can also be affected.
If this sounds familiar then you may be one of the thousands of people suffering from intermittent claudication.
Intermittent claudication is pain in the leg that comes on when the muscles are working, caused by narrowing of the arteries supplying the muscles with blood. This “furring-up” of the arteries is all part of ageing, but in some people the process is greatly accelerated. We know that cigarette smoking, high blood pressure, raised cholesterol and diabetes can all play a part. One in five men over 50 is thought to have some degree of intermittent claudication but women can also be affected.
Your GP should be able to tell you if the pain in your leg is intermittent claudication. If you get pain in the muscle of your calf or thigh when you walk, pain that comes on sooner when you walk more quickly or walk up hill, but eases after a few minutes rest – then go and see your doctor. He or she will need to know exactly how far you can walk before the pain stops you, and will need to examine your legs and feel or listen for foot pulses.
If you do have blood flow problems what does it mean and what will happen next? First of all if you smoke you must stop immediately – nicotine and carbon dioxide inhaled from tobacco smoke damage blood vessels, reduce the amount of oxygen blood can carry and constrict small blood vessels. Your doctor may suggest you take an aspirin every day, aspirin helps by thinning the blood. A referral to a Vascular Surgeon or a Vascular Laboratory may also be suggested.
The Royal Sussex County Hospital in Brighton has one of the busiest Vascular Laboratories in the UK, the technicians at the laboratory can perform a range of tests to confirm intermittent claudication and pinpoint the arteries involved. These tests are painless and do not involve any needles or injections. Most patients seeing a Vascular Surgeon will be examined, have a blood test, be warned again to stop smoking and advised what they can do to help themselves. If the arterial narrowing is advanced then x-rays of the arteries may be needed. There are no pills that can make the problem go away but there are treatments that can help stop the condition progressing. If the arteries are blocked then bypass surgery may be the only option.
Intermittent claudication can be serious, left unchecked it can lead to amputation. Occasionally it can be acute and when a patient is suspected of having an acute occlusion the case must be discussed immediately with a Vascular Surgeon who will refer to the Vascular Laboratory for initial assessment. The speed of this assessment and the hours saved by the immediate availability of a Vascular Laboratory can make the difference between death, loss of leg or complete recovery of limb function to normal after treatment. The rehabilitation after amputation can take many months and only a few walk successfully with their artificial limbs.
By Simon Ward
Chief Technologist
Vascular Assessment Unit
Royal Sussex County Hospital
Brighton
Who says that your legs don’t swell on long flights!
There has been much recent media coverage about the risk of developing a DVT (deep vein thrombosis) whilst flying on long haul flights and this has become known as “Economy Class Syndrome”.
Deep vein thrombosis cartoon
Who says that your legs don’t swell on long flights!
Veins carry blood from the tissues to the heart. In the legs, the superficial veins (which sometimes develop into varicose veins) collect blood from the skin, whilst much bigger veins – the deep veins – are situated within the muscles. During exercise the blood flow to the muscles increases and the volume of the flow in these deep veins (squeezed out as the muscles contract) is very large, whereas at rest the flow can be sluggish.
In order to stop us bleeding if we are injured, there is a complex coagulation system which converts liquid flowing blood into jelly like clots which block the damaged blood vessels thereby plugging the leak. This may be life saving but in certain circumstances blood may clot within normal blood vessels causing a “thrombosis”. This can occur if blood flow is reduced for long periods and this is why deep vein thrombosis used to be common after surgery when patients were immobilised in bed for long periods. Fortunately this is now uncommon since we use anti coagulant drugs to reduce clotting and we also get people moving quickly to increase the flow in their veins.
Other factors also increase the tendency for thrombosis. These include some drugs and increased viscosity (thickness) of blood.
What happens in DVT?
Blood clots in the deep veins cause the leg to swell as fluid leaks out into the tissues. This is often very painful. The clots develop first in the calf but may extend into the veins in the thigh or even up into the very large Iliac veins in the pelvis. Sometimes if appropriate treatment is started early, the clots will dissolve but this may still leave the veins permanently damaged leading to prolonged swelling and sometimes leg ulcers many years later.
The most dangerous effect however is Pulmonary Embolus where the clot becomes dislodged from the legs and rushes up through the abdominal veins into the heart. The clot may then lodge in the large pulmonary arteries blocking flow to the lungs. This usually causes severe chest pain with sudden collapse and may be fatal. This catastrophe may occur as the passenger gets up after many hours on the plane and walks to the terminal. Sometimes, however, swelling may start some days after the flight and collapse may follow. These cases are seen away from hospitals close to airports and in the past the connection may not have been realised!
Some things increase the risk for an individual. These include obesity and previous history of DVT. Women taking the contraceptive pill are always at a slightly higher risk of thrombosis, and HRT may marginally increase the risk. Flying should be avoided for some weeks after surgery.
What increases the risk?
Although DVT can occur after any form of travel the evidence that flying is a real risk is mounting and indeed would be expected to take in to account the factors listed above.
Why is there an increased risk?
If we now imagine ourselves on a long flight there are a combination of factors which will increase the risk of a DVT!
Firstly in the sitting position, particularly if there isn’t much room and our knees are bent, flow in the deep veins is restricted. If we sleep for long periods without moving the danger is even greater.
Secondly, we often become dehydrated when flying the cabin air is warm and dry and alcohol encourages excess fluid loss. This blood may become thicker than usual.
There is also the possibility that cabin pressure may have an effect on clotting. At normal cruising altitude (30,000 feet) you couldn’t breathe outside the plane the air pressure is too low. Within the cabin air is pressurised to approximately the same as 7,000 feet allowing us to breathe comfortably. The air at this altitude is, however, much thinner than at ground level; as you would know if you have ever skied at this height.
Can the risk be reduced?
Simple measures like drinking quantities of non alcoholic liquids during the flight (have a bottle of spring water with you). Get up and move around the cabin as often as you can and waggle your feet up and down when in your seat – This is a great way to increase vein flow! Wearing support stockings may help.
Aspirin is very effective in reducing the risk of clots. A junior aspirin daily starting some days before travel might be advisable, particularly if you are at high risk. But remember that this may be dangerous if you have had a stomach ulcer or problems with abnormal bleeding in the past.
Will I ever dare fly again?
The biggest danger in air travel is still overwhelmingly road accidents during the trip to the airport. Tens of millions of people fly long haul every year and very, very few of them get a DVT.
“Forewarned is forearmed”, and a few simple precautions may make all the difference. Enjoy your trip.
What to do if I am worried?
Ask your doctor before the trip if you think you might be at increased risk of DVT, or indeed if you are fit to fly if you have other medical problems. Conditions on board are very different from ground level and people with heart or chest problems may need advice. Diabetics may also need to change the timings of their medication.
If your doctor thinks you may have developed a DVT he could send you to the new Vascular Assessment Unit at the Royal Sussex County Hospital. All the equipment in the Unit has been provided by The Sussex Stroke & Circulation Fund through donations from the public. The most recent purchase is a “state of the art” Duplex ultrasound machine – this will diagnose a DVT immediately and painlessly without any unpleasant injections. If the test is positive treatment can be started immediately and further problems avoided.
By Paul Hurst BSc, MS, MRCP, FRCS
Consultant Vascular Surgeon
Royal Sussex County Hospital
Brighton